
ACMS MIPS Resources
Resource List
Click a section below to jump to it.
- I: Medicare Payment Overview
- II: What is MIPS?
- III: Participate in MIPS
- IV: QCDR - MohsAIQ
- V: 2021 Reporting
- VI: APMS
I. Medicare Payment Overview
The Medicare Access and CHIP Reauthorization Act (MACRA) was signed into law April 2015, repealing the flawed sustainable growth rate (SGR) and establishing a two-track Medicare physician payment system that emphasizes the transition to value-based payment and delivery. To implement MACRA, the Centers for Medicare and Medicaid Services (CMS) established the Quality Payment Program (QPP), whereby eligible clinicians will either participate in the Merit-based Incentive Payment System (MIPS) or join an Advanced Alternative Payment Model (APM).
With few APM options available for Mohs surgeons, the American College of Mohs Surgery (ACMS) created MohsAIQ, a CMS-recognized Qualified Clinical Data Registry (QCDR) that allows Mohs surgeons to participate in the MIPS track of QPP by reporting quality measures relevant to their practice.
II. What is Merit-based Incentive Payment System (MIPS)?
Performance Categories, Weights and Thresholds

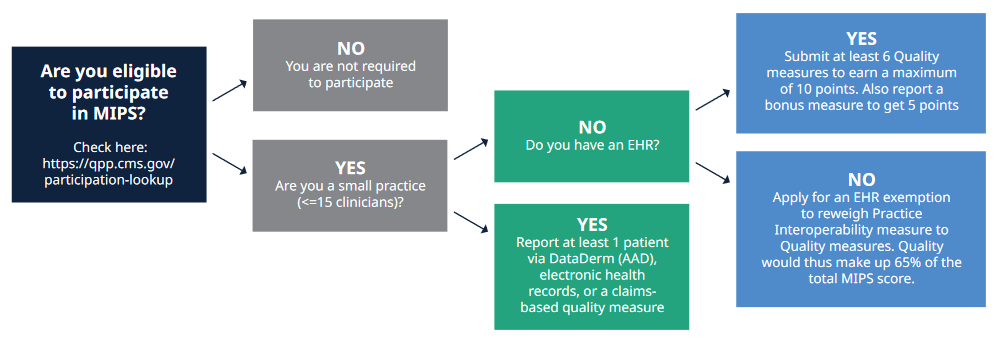
MIPS incorporates four weighted performance categories – Quality, Cost, Promoting Interoperability, and Improvement Activities – that contribute to an annual MIPS final score of between 0 and 100 points. If you score 60 points, you will avoid the 9% penalty. A score of 61-84 points qualifies you for the minimal incentive. A score of 85-100 points qualifies you for a 9% maximum incentive.
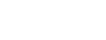
MIPS Eligibility
Are you eligible to participate in MIPS? Check here: https://qpp.cms.gov/participation-lookup
III. MIPS Participation
Brief Overview on Eligibility
Clinicians may participate in MIPS as individuals or as a member of a group (or virtual group). Individual clinicians (i.e., a single NPI tied to a single TIN) will have their payments adjusted based only on their performance. Clinicians that report as part of a group (i.e., identified by their NPI, who share a common TIN) will have their payments adjusted based on the group’s performance across all four MIPS categories.
Clinicians may also participate as a “virtual group,” which is a combination of two or more TINs made up of solo practitioners and groups of 10 or fewer eligible clinicians who come together virtually (regardless of specialty or location) to participate in MIPS for a performance period of a year. Learn more about this option by reviewing CMS’ Virtual Groups Toolkit.
Reporting Mechanisms
Clinicians may also choose to collect quality data via multiple mechanisms, including claims (limited to physicians in small practices), registry (i.e. MohsAIQ), certified electronic health record (CEHRT), and web-based attestation (via the QPP Portal). Clinicians may use different mechanisms across performance categories (e.g., report quality measures via claims and improvement activities via registry) and within performance categories (e.g., report quality measure A through claims and quality measure B through a registry).
IV. QCDR - MohsAIQ
Clinicians can choose to collect quality data via multiple mechanisms. Clinicians may use different mechanisms across performance categories (e.g., report quality measures via claims and improvement activities via registry) and within performance categories (e.g., report quality measure A through claims and quality measure B through a registry).
Options for MIPS reporting are outlined below. There are several options available to physicians and groups.
ACMS members are strongly encouraged to report quality data using MohsAIQ, a CMS-recognized QCDR approved for 2021, but are also encouraged to report additional quality measures through multiple mechanisms if able to do so. When multiple mechanisms are used to report quality measures, CMS will aggregate the measures and count the most highly scored measures.
Reporting Options:
A. Medicare Part B Claims
- No additional administrative cost; affordable
- Only available to solo practitioners and small practices (<15 eligible clinicians (ECs))
- Quality data codes/G-codes may be reported by billing staff or billing companies
- Only available for the quality category for certain measures (not an option for reporting all MIPS measures)
B. Log-in and Upload or Attest via CMS QPP Submission Portal
- Affordable options
- Must have HCQIS Access Roles and Profile (HARP) system account
- ECs can attest and upload their electronic files from an HER qualified registry, or QCDR for the categories
- More real-time scoring provides insight into performance
- Attestation does not require submission of data
C. Qualified Clinical Data Registry (QCDR)
- Examples: MohsAIQ, DataDerm
- Most MIPS measures are reportable via registries and QCDR
- QCDR include MIPS and non-MIPS measures (eligible for MIPS credit that can be specialty-specific and may be more applicable to some physicians/ECs)
- Participants often must pay registration fee and additional costs (varies per vendor)
- Some national specialty societies offer registry/QCDR at no or low cost
- Performance feedback may be provided within performance period
- Difficulty linking to EHR systems for automatic extraction of data
- Manual data entry option may be time consuming
D. Electronic Clinical Quality Measures (eCQM) / MIPS Clinical Quality Measures (MIPS CQM, previously named “Registry Measures”)
- In MIPS program, there are sereral different sets of measures available for Quality category
- eCQM and MIPS CQM are “collection types” for Quality category data requirements
- MIPS CQM
- ECs document data in the medical record., either electronically or on paper as part of routine documentation during care delivery
- Structured data capture not required, digital data often transcribed after dictation
- ECs or abstractor reviews data documentation for each qualifying patient. Documentation can be combo of electronic and paper documentation.
- Based on abstractor’s answers to measure algorithm, patient either meets performance components or does not. Measure performance score based on aggregate result of all patients qualifying for the measure.
- ECs most commonly choose MIPS CQMs if there are not enough measures relevant to their specialty to meet minimum reporting requirement
- Down side is continued abstraction burden and lack of timely results to ECs for performance improvement
- MIPS eCQM
- Using measure specifics, eCQM data elements are built and mapped to code sets for capture within the HER
- ECs document data electronically at point-of-care which is captured in HER
- Software identifies which patients/encounters qualify for measure, software determines whether patient meets or fails performance
- Data review performed after all calculations have been completed by software. Performance improvement activities based on frequent review of measure and provider results.
- Provide near real-time reporting and have less costly ongoing maintenance
- When submitting as a group, results are applied at group level (if some specialist ECs cannot find measures applicable to them, they can get credit for other ECs eCQM performance within the group)
E. Certified Electronic Health Record Technology (CEHRT)
- Many practices already use EHR in daily practice
- Convenient collection of data captured directly from CEHRT system
- CEHRT vendors may submit data on ECs behalf, but EC must trust that vendor will correctly and accurately submit the information
- Limited availability of applicable quality measures that can be reported via CEHRT
F. CMS Web Interface
- Only available for groups of 25 or more ECs
- Higher reporting thresholds for quality measures (must report more data on more measures)
- Must register with CMS by June 30, 2021
- May enter data manually or upload data directly from EHR system
G. Consumer Assessment of Healthcare Providers and Systems CAHPS) for MIPS Survey
- Measures 10 key domains of patients’ experience of care that are referred to as SSMs (Summary Survey Measures)
- Administered via Mixed Mode data collection protocol including: CMS pre-notification letter, 2 survey mailings, up to 6 follow-up phone calls to patients who don’t return a survey by mail.
- Takes place of one quality measure for MIPS quality category
- Must register with CMS by June 30, 2021
- Must pay CMS-certified survey vendor to conduct CAHPS for MIPS survey
- Must be reported in conjunction with another reporting mechanism
V. 2021 Reporting of MIPS
2021 Final Scores and 2023 Payment Adjustments
How to Earn a Positive Payment Adjustment and an Exceptional Performance Bonus
- Decide whether to apply for the hardship exemption to have PI re-weighted to Quality
- Earn 15 points by fully participating in the IA component
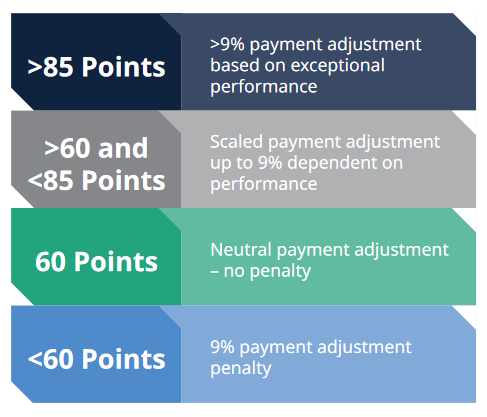
2021 MIPS Performance Categories
The maximum downward payment adjustment in 2023 is -9 percent based on 2021 performance. To avoid this penalty, Mohs surgeons must at least earn a total MIPS score of 60 points – the performance threshold for 2021.
CMS Resources:
VI. Alternative Payment Models (APMs)
Congress passed MACRA to incentivize participation in Alternative Payment Models (APMs). MACRA also created a second payment pathway, MIPS, for those not in APMs. MIPS was intended to be an on-ramp to APM participation.
An APM is a new payment approach to paying for medical care:
- Most often APMs utilize reimbursement methods that are different from traditional fee-for-service payments. However, APMs may retain fee-for-service payment elements as part of reimbursement structure.
- APMs require healthcare organizations (often hospital and affiliated physician practices) to align themselves with the goal of taking better care of a population of patients.
- Focus is on delivering higher quality of care rather than on the amount of care being given.
- APMs hold providers accountable for achieving specific quality performance goals in an efficient manner.
- Group practices participating in an APM receive added incentive payments to achieve the stated goals.
A common example of an APM is a Medicare Shared Savings Plan (MSSP), a.k.a. Accountable Care Organization (ACO). Under MSSP, if organization can realize savings by providing high-quality, low-cost care to a defined group of Medicare beneficiaries seen by the MSSP providers, Medicare will share savings with the ACO.
“Advanced APMs” are a subset of APMs that qualify for MACRA’s second payment track:
- Offers physicians and group practices incentives to provide high-quality, cost effective care under payment models that move away from fee-for-service payment system
- Providers must be in a qualifying Advanced APM and become a qualifying participant (QP) by achieving threshold levels of payments of patients
- Requires participants to use certified EHR technology
- Base payment on quality measures comparable to those in MIPS quality performance category
- Often require APM entities to bear more than nominal financial risk for monetary losses related to patient outcomes
- Advanced APM incentives:
- QPs receive an annual 5% lump-sum payment bonus, based on previous year’s Medicare part B payments. Bonus applies in payment years 2019-2024
- QPs are exempted from MIPS participation and payment adjustments
- Model-specific awards can also be designed within an APM framework